
Executive function in neurodiverse children
An illustrative description and approach of the executive function network in neurodiverse children
The description that follows here has been simplified in order to make it more understandable to the general public. A significant amount of complex anatomy, neurology, and neuropathology has been excluded.
The executive function network includes specific localized areas, i.e., the prefrontal cortex, neocortex, limbic system, basal ganglia, and the motor cortex. Each one of these has a specific role to play in the execution of an order. Thus when confronted with selective or combined malfunctioning of these areas, the execution is inhibited in a lesser or more complex manner.

The various regions of the brain.
1. Prefrontal cortex
The prefrontal cortex operates as the “business manager “ of the brain. It receives information via the senses (hearing, vision, touch, taste, and smell) and then has to process them in order of importance. This is the area where the sorting out of information takes place, usually at a very fast rate. The prefrontal cortex is bombarded with millions of information bits per second, so one can imagine that if the filtering of the information is not efficient, then information overload will result, which makes it very difficult for the individual to concentrate on a specific challenge - for example a mathematical computation. Two chemicals or neurotransmitters play an important role in supporting the filtering of information, namely dopamine and noradrenaline, of which the former is the most important. As an example, the individual is requested to add 7 plus 11. Given that the prefrontal cortex has sufficient neurotransmitters, it will avoid all other sensory input and focus on the question at hand. It will then pass the question on to the neocortex to be processed. The working memory operates as a rapid access memory where initial programming might take place, but as soon as prefrontal cortex is satisfied with the result, the information is passed on to the neocortex.
2. Neocortex
Once the information is received by the neocortex from the prefrontal cortex, the processing takes place. As an example, the neocortex will then calculate the answer to be 18 and will then be transferred to the basal ganglia.
3. Basal ganglia
The function of the basal ganglia is to sort out what happens to any information received e.g. whether it needs further computation such as being processed by the speech machinery (Broca’s speech area) in order for the mouth to form the word “eighteen”, or sent directly to the motor cortex to inform the hand to write “18”.
4. Motor cortex
The motor cortex is responsible for all mechanical performances, such as walking, running, talking, and writing. One can imagine that if the motor cortex is effectively controlled, these functions will be fluent and effective. So writing will be eligible, speaking will be clear, and running will be controlled - especially when the individual is required to sit still and concentrate. On the other hand, when not, then it will result in some disorder such as the handwriting being illegible, an “always on the go” tendency, and a significant amount of “unnecessary” movements such as an inability to sit quietly, feet tapping, making funny noises, or fidgeting.
5. Limbic system
The limbic system is a group of neurons that contains the emotional area. Via constant monitoring of what’s going on around in the brain, it will support the individual’s emotions by either boosting the confidence and self esteem (giving feedback to the prefrontal cortex) or in the case of things not matching up to the individual’s potential, will result in an increase in anxiety and loss of self worth.
6. Cerebellum
Although not on the same level of importance as the executive function network in delivering the information to the motor cortex, the cerebellum plays a very important role in controlling hand, eye, and body movements, as well as coordination. For any order to be carried out, the cerebellum will integrate all movement in a coordinated manner with the eyes and constantly monitor feedback until the required response has been delivered.
7. Neuroplasticity
From the moment of birth, the brain has the ability to develop billions of neurons with interconnections between themselves. Depending on stimulation, these neurons will strengthen the connectivity, so called neuroplasticity, strengthening the stimulated pathways and thus improving functionality. The capability to support neuroplasticity will continue into the third decade. It is extremely important to facilitate neuroplasticity through the introduction of certain support programs such as speech, occupational and remedial therapy, but also with certain medications that will augment the speed at which these neurons will grow and strengthen.
8. Target domains
Motor hyperactivity and inattention:
Following the international guidelines as set out in the DSMV directive.
The aim is supporting patients to increase their concentraction and focus and decrease their hyperactivity.
Irritability (aggression, self-injury, tantrums):
Typically the irritability will follow on an underlying anxiety.
The focus will be to decrease these symptoms in order to improve communication.
Restrictive, repetitive patterns of behaviour:
Underlying to the above is an anxiety that drives the repetitive behaviour whereby the comfort is increased.
Disrupting the behaviour often leads to severe aggression.
The aim is to lessen anxiety and stabilise the mood.
Sleep disturbance:
Poor sleep patterns often lead to severe mood disruptions during the day
The aim is to improve early onset of sleep as well as a sleep time.
Mood disorders:
Mood disruptions are the result of uncontrolled anxiety that, again, stems from poor or ineffective communication.
Focussing on improving internal neural communication results in the stabilization of mood.
Anxiety disorders:
Up to 45% of patients suffer from underlying anxiety to a greater or lesser extent.
It is critical to manage anxiety which then often leads to the normalization of a number of symptoms such a aggression, irritability and concentration problems.
Communication disorders:
Verbal or non-verbal (eye contact avoidance, not responding to a request) communication issues are mostly related to internal message related problems.
It is quite important to exclude hearing deficits.
Specific speech deficits should be identified.
Early identification and treatment will result in improvements as the brain is capable (neuro-plasticity) to build additional neural networks.
Motor coordination disorders:
These disorders can be attributed to central (inside the brain), nerve, and/or muscle related problems and therefore it is very important to identify the cause of any motor coordination issues.
Occupational support is critical in strengthening this weakness.
9. Different pathologies
Attention Deficit Hyperactivity Disorder (ADHD):
The DSMV contains an excellent description of the classification. Basically, it boils down to the inability to concentrate or focus and might include hyperactivity.
Oppositional Defiant Disorder (ODD):
As a co-morbid association of ADHD, ODD includes children that struggle to accept requests given by caretakers or educators.
Conduct Disorder:
Abnormal behaviour such as hurting animals, aggressive tantrums, and spitefulness.
Anxiety & Depression:
Where stress involves emotional behaviour that includes concern and worry, but will be relieved as soon as the stressor is removed, anxiety remains despite lessening of the stress factors. Depression includes anxiety but then deteriorates where normal social and physiological functions such as sleep, appetite, and drive is affected.
Dyslexia:
A difficulty reading due to problems identifying speech sounds and how these sounds relate to words and letters. This will then also affect the ability to write.
Autistic Spectrum Disorder (ASD):
A development disability that affects the internal communication pathways of the brain resulting in the patient struggling to understand social cues and norms as well as making effective verbal communication.
Pathological demand avoidance (PDA):
PDA (now known as exessive demand avoidance (EDA)) is a developmental disorder. It is a complex and misunderstood condition that includes the everyday resistance to normal demands made by caretakers and educators. Severe anxiety seems to be the underlying driver that leads to the resistance.
Tourette syndrome:
Tourette syndrome includes the inability to control repetitive movements and/or sounds (tics). In layman’s terms, it involves a highly intelligent and talented brain that finds it difficult to control the body it inhabits.
10. Therapeutic approach
Physical examination:
It is very important to conduct a thorough physical examination to exclude ailments that might be unrelated to the mental or physiological problems, such as diabetes, iron deficiency, or endocrine disorders e.g. an underactive thyroid or heart abnormalities.
Diagnosis:
Reaching a definitive diagnosis is extremely important to both the caretakers and educators as it will support the effective treatment but also limits present problems.
Level of functionality:
Determining the level of functionality will enable the caretakers to reach consensus on the expectations and road ahead and will also enable the educators and supporting team (occupational, speech and play therapists as well as psychologists) to plan and execute an appropriate educational program.
Partnership with caretakers:
Bringing the caretakers on board as to the specific diagnosis, treatment options, and the educational, physical, and emotional needs of the patient is very important in order to reach an effective and comprehensive strategy.
Approach to pharmaceutical choices:
The choice of medicines depends on basically four options. How to improve concentration, improve internal communication, lessen anxiety including depression, and stabilise mood.
Feedback:
Regular feedback is critical for effective management and monitoring of the response to the medication. The Tracto App was developed with this in mind as it supports caretakers to monitor a number of factors such as emotional status, concentration, behaviour, and sleep.
11. General interventions
Physiological support:
Initial physiological assessment will enable caretakers to understand the potential and limitations of the patient’s capacity to handle everyday physical, social, and educational challenges. Ongoing physiological support is often required to enhance and monitor progress of the above-mentioned challenges.
Occupational therapy:
As an adjunct to physiological support, occupational therapy focusses more on functional deficits such as writing, hand-eye coordination, and balance gait deficits.
Speech therapy:
Specifically with all speech deficits, the role of the speech therapist is to improve the neural integration between word recognition and sound modulation.
Remedial support:
A number of remedial support programs should be made available to optimise the patient’s potential with regards to the physical, auditory, vision, tactile sensitivity, speech, and intellectual limitations.
Scholastic:
Determining and advising on the educational limitations as well as which educational program and setting will best support the specific needs of the patient should be a very important and critical milestone in the support armementarium.
Exercise:
Nothing beats regular exercise when it comes to improving emotional and physical wellbeing. Caretakers as well as the patients themselves should be encouraged to follow a healthy exercise program.
Physical support:
Supporting patients with physical limitations is critical in order to optimise their intellectual capacity.
12. Pharmaceutical interventions
Stimulants:
Methylpenidate (Ritalin, Contramyl, Concerta, Neucon, Mefedinel, Radd) increases the dopamine levels in the prefrontal cortex whereby concentration is actively enhanced. Its action is almost immediate and, depending on which one is being used, it will be effective for 4, 8, or 12 hours. Side effects include loss of appetite and struggle to fall asleep.
Lisdexamfetamine (Vivanse): Its action lasts for 14 hours. It has less side effects compared to methylphenidate.
Non-stimulants:
Atamoxetine (Inir, Attentra) increases noradrenaline in the prefrontal cortex. It takes significantly longer to be effective with the first signs of increased concentration around 3 weeks and optimum effect around 6-8 weeks. It works for 24 hours and theoretically has no side effects.
Anti-psychotics:
Anti-psychotic drugs has a number of beneficial effects especially decreasing irritability, stabilising mood, and improving behaviour. One of the most important benefits is that it improves internal communication whereby speech and cognition is improved.
It’s important to administer the medication during the periods when communication is optimal, e.g. during school as well as during the early evening between 16:00 and 21:00. It is also effective in controlling tick disorders.
Its effect usually starts within 1 hour and lasts from 8 (respiridone) to 12 (aripiprazole) hours.
Side effects include drowsiness and weight gain. Newer options such as Rexulti and Geodon has less side effects.
Anti-depressants (anti-anxiety agents):
Selective Seretonin Reuptake Inibitors (SSRI) such as Sertraline etc. increase serotonin in the emotional area (limbic system). Side effects are minimal but could include drowsiness and weight gain.
Monoamine Oxidase Inhibitors (MAOI) such as Ethipramine are less effective, but has other beneficial effects such as an increase in concentration.
Stresam (Etifoxine) is highly effective in managing short term anxiety with no sedative effect.
Mood stabilizers:
These drugs all fall under the anti-epileptic range (sodium valproate, carbamazapine and lamotrigine) and are used to stabilize the mood in patients where mood fluctuations leads to social and educational disruption.
Alpha-2 agonists:
A very inexpensive and effective option to improve concentration and stabilise mood. In higher concentrations it also induces sleep.
Lithium:
Lithium (Camcolit) is a potent mood stabiliser and because of its unique action, it is classified alone.
Sedatives:
These drugs all fall under the benodiazapine classification, e.g. Valium, Ativan, Rivotril, Xanor, and Urbanol are a few well known brands. They are highly effective but addictive in the long run, excluding Urbanol. Side effects are drowsiness and may lead to depression.
13. Neurofeedback
Neurofeedback involves the measurement of certain brainwaves via electrodes placed on the head while the patient is concentrating on a program or game on a computer screen. By “forcing” the brain to focus over a period of time and repeating this program weekly for about six months, the brain will learn to adapt to the stimulus and become more focused. The application varies but includes improving concentration, lessening anxiety, and improving cognitive functioning.
At the present time, neurofeedback is available at specific sites in South Africa but requires the patient to visit the site twice weekly and is quite expensive. A new option will be introduced in the latter part of 2025 (Neeuro) where the patient can take the headband home and monitor via a laptop or tablet device.
14. Immunoglobulins
Following international oberservations there is a rapid increase in the incidence of children on the autistic spectrum (ASD) in South Africa. Likewise, children with PANDAS (paediatric autoimmune neuropsychiatric disorder associated with A Streptococcal infection) are also on the rise. Personal observations of both these neuropathologies have been met with an upsurge that is both disturbing and challenging.
A large amount of research has gone into understanding the neurobiology of both entities. Clearly, an underlying autoimmune derangement is at play here. It has been demonstrated that in some children with autism, an abnormal gut microbiome played a role in triggering an autoimmune response. There again, in PANDAS, the basic underlying inflammatory processes causing the derangement of the basal ganglia are the result of antibodies directed against the latter.
Thus, the question arises whether a cross link exists between the two pathologies. Intitial results indicated that around 17% of children with ASD could have underlying PANDAS. Again, it seems that this co-arrangement is on the uprise.
Management for both pathologies are very similar with the aim being addressing the target symptom domains i.e. concentration, irritability, OCD, ticks, mood disorders, and anxiety. Psychological interventions seem to be limited whereas there is a move towards pharmacological support. IVIG has recently been demonstrated to have a dramatic effect in PANDAS where in ASD it has not been so effective. One reason may have been the timing of the intervention as with ASD the neural apoptosis has already taken place by the time IVIG was instituted. The rationale behind the administration of IVIG is based on the effect it has on the neuroinflammation that exists in children with either enities.
In the developing world, the exhorbitant cost of IVIG excludes most patients from the benefit. Recently a program administering intramuscular immunoglobulins (Intragam) for PANDAS has demontrated a surprising advantage in curtailing the severity of ticks. Although anecdotal, it opens up a cost-effective opportunity to administer pooled immunoglobulins to a wider population. At the same time, it might also lead to the administration of immunoglobulins as an early intervention for children with profound ASD.
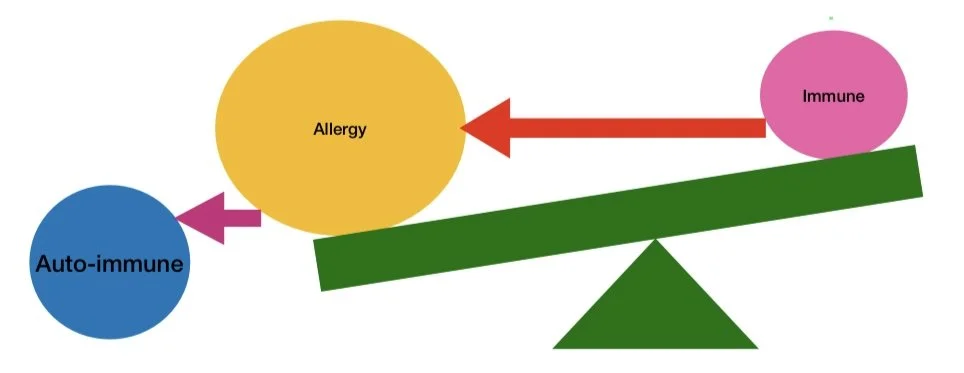
15. Imbalance on auto-immunity
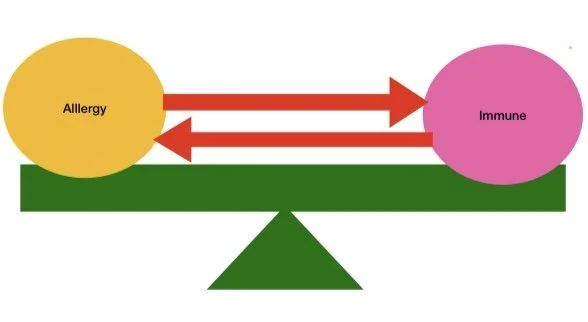
The balance between allergy related symptoms, the immune system, and auto-immune diseases has extensively been discussed in numerous research publications. The hygiene theory, supported by an equal amount of information, indicate that there has been a shift away from a Th1 (attacking bacteria) to a Th2 (responding to allergens) reponse potentially caused by the industrialisation, overuse of antibiotics, and our under exposure to unrefined nutrients and soil bacteria. This is backed up by changes in the gut commensal of infants born via the ceasarian route. The balance between the immune system and sensitivity to allergies depends on the exposure to sepcific allergens. The more allergic, the more the balance moves towards an “allergic overweight”. Finally the system moves sofar towards an allergic overweight that the immune system becomes deranged and starts “attacking” the body, the so called auto immune reaction.
The recent increase in auto-immune diseases has been characterised by a parallel increase in the neurodiverse population with autism leading the pack and paediatric acute onset neuropsychiatric syndrome following suite. Although a direct causal relationship is difficult to establish, research has demonstrated the presence of neuro-inflammation as a result of an increase in the Th2 response. In layman’s terms it means that our body has moved from a defensive mode to a reactive mode attacking outside invaders (allergens) and in extreme cases turning onto our own cell surface antigens (auto-immune). Behavioural changes should be instituted as early as possible including more natural and home births, often playing outside thereby increasing exposure to soil bacteria, and increase in uncooked nutrients such as vegatables and fruit. Optimisation of the iron levels, the vitamin D status, and adequate intake of essential B vitamins such as folic acid and cyanocobalamin should be included in the realignment of our immune system.
In the case where a change in the allergy status (IgE increase) and/or decrease in the immune system response (decrease in IgA and IgG) can be demonstrated, the challenge will be to decrease exposure to the offending allergens (dietary and environmental avoidance) and an improvement in the immune response through natural interventions such as echinacea. If this proves to be unsuccessful, then pharmacological agents such as antihistamines, leukotrine receptor blockers, and in serious cases pooled immunoglobulins should be considered and administered.
Obviously it becomes a challenge once the neuro-inflammation has already led to structural neural changes and apoptosis. Fortunately the brain demonstrates neuroplasticity up to the third decade, aiding in combatting the neural onslaught. Therapeutic modalities such as neuro-feedback have demonstrated some benefit whereas pharmacological agents e.g. sodium valproate, selective serotonin re-uptake inhibitors, and prefrontal cortex stimulants have clear benefits in improving neural conductivity. The future star wars will be aimed at our own immune system and hopefully we will see a return to a more natural and healthy way of living. In the meantime, we will have to make use of all the means we have at our disposal including the drug armamentarium mentioned above.
